St. Paul Nursing Home Violation Registry
A structured guide to the public-record violation categories and regulatory findings that apply to Minnesota nursing facilities. I publish this registry so any family researching institutional care in Saint Paul or elsewhere in Minnesota has a working map of what the state tracks, what the federal inspectors record, and what the clinical signatures of neglect look like when a case later needs to be built.
Scope note: The registry data is anchored to Saint Paul and Ramsey County facilities. The framing and methodology apply statewide to any Minnesota nursing home, assisted-living facility, or home-care setting covered by Minn. Stat. Ch. 144A or the Assisted Living Bill of Rights at Minn. Stat. §§ 144G.90-.91.
Dataset Overview
What This Registry Tracks
When a family suspects that a parent or grandparent has been harmed inside a Minnesota nursing facility, the first problem is not legal. It is informational. The regulatory record lives across several public systems — the Minnesota Department of Health Office of Health Facility Complaints, the federal Centers for Medicare & Medicaid Services Care Compare file, county adult protection filings — and none of them read like a single registry. This page consolidates the categories those systems use and maps each category to the clinical signature and the statutory framework behind it.
The goal is practical. A family researching a facility before placement, or a family working backward from a harm event, should be able to see what is being tracked, where the public record lives, and which categories correspond to the objective medical findings that turn a subjective concern into a documentable claim.
- Primary use: help families map a concern about institutional care to the specific regulatory category that governs it.
- Spatial coverage: Saint Paul and Ramsey County facilities, with statewide regulatory framing.
- Source categories: Minnesota Department of Health Office of Health Facility Complaints investigative reports, CMS Care Compare federal survey data, Ramsey County adult protection filings, published state oversight reports.
- Row integrity rule: categories listed below come from named public-record frameworks. Specific facility findings are not reproduced on this page. Families can search them directly at the MDH and CMS public portals.
- License: Creative Commons Attribution 4.0. Free to use with attribution.

Registry Structure
Violation Categories Tracked Under Minnesota Oversight
The categories below are the ones the Minnesota Department of Health and the federal CMS inspectors use when they investigate a complaint or conduct a recertification survey. Each category ties to a statutory framework and to a clinical or operational signature that is visible in the medical record once a family requests it under Minn. Stat. §§ 144.292-.293.
| Category | What It Covers | Governing Framework | Clinical or Operational Signature |
|---|---|---|---|
| Maltreatment — neglect | Failure to provide adequate care, supervision, nutrition, hydration, hygiene, or medical attention. | Minn. Stat. § 626.557 (Vulnerable Adults Act); Minn. Stat. Ch. 144A | Pressure injuries, weight loss, low serum albumin, dehydration labs, recurrent urinary tract infections. |
| Maltreatment — physical abuse | Physical injury inflicted by staff, another resident, or a visitor admitted to the facility. | Minn. Stat. § 626.557 | Bruising patterns inconsistent with stated cause, fractures without witnessed fall, skin tears with staff-hand signatures. |
| Maltreatment — sexual abuse | Any non-consensual sexual contact. Vulnerable-adult capacity is presumed compromised for most residents. | Minn. Stat. § 626.557 | Forensic examination findings; behavioral-change documentation in nursing notes. |
| Maltreatment — financial exploitation | Unauthorized use of a resident’s funds, property, or benefits by staff, a guardian, or a family member with access. | Minn. Stat. § 626.557 | Bank withdrawal patterns; unexplained asset transfers; missing personal property. |
| Medication administration | Wrong medication, wrong dose, wrong route, wrong time, or omitted dose. Also covers unmonitored high-risk drugs. | Minn. Stat. Ch. 144A; federal 42 CFR § 483.45 | Medication administration record gaps, adverse drug events, hospitalizations for drug toxicity or under-treatment. |
| Falls and fall prevention | Failure to assess fall risk, implement the care plan, or respond to a fall with appropriate medical evaluation. | Minn. Stat. Ch. 144A; federal F-tag 689 | Unwitnessed falls; fracture patterns; delayed imaging; traumatic brain injury findings on 3-Tesla MRI that a 1.5-Tesla scanner missed. |
| Pressure injuries | Failure to reposition, off-load pressure, maintain nutrition and hydration adequate to skin integrity, or monitor for early stage breakdown. | Federal F-tag 686; Minn. Stat. Ch. 144A | ICD-10 L89 staging, wound-care notes, Braden Scale documentation, admission-versus-in-facility acquisition record. |
| Infection control | Failure to implement standard precautions, isolation protocols, or outbreak response. Includes catheter-associated infections. | Federal F-tag 880 | Recurrent urinary tract infections, sepsis admissions, cluster patterns of respiratory infection. |
| Staffing | Inadequate nurse and nurse-aide coverage, unlicensed staff performing licensed tasks, failure to meet the care-hours standard. | Minn. Stat. Ch. 144A; federal F-tag 725 | Missed medication passes, delayed call-light response, documentation gaps that correlate with staffing shortages. |
| Resident rights | Failure to respect dignity, privacy, informed consent, freedom from unnecessary restraint, or the right to be free from retaliation. | Minn. Stat. § 144.651 (Health Care Bill of Rights); Minn. Stat. §§ 144G.90-.91 (Assisted Living) | Chemical and physical restraint patterns, care-plan consent documentation, grievance-log entries. |
| Discharge and transfer | Involuntary discharge without notice, refusal to readmit after hospitalization, or transfers that violate resident-choice protections. | Minn. Stat. Ch. 144A; Minn. Stat. §§ 144G.90-.91 | Discharge-notice documentation, hospitalization-return records, family-communication logs. |
Reading the table: the rightmost column is the clinical-correlation column. It names the evidence that, once a family obtains the medical record, converts a category label into documentable harm. That mapping is the Pillar II work.
Regulatory Framework
Minnesota Statutory Timeline
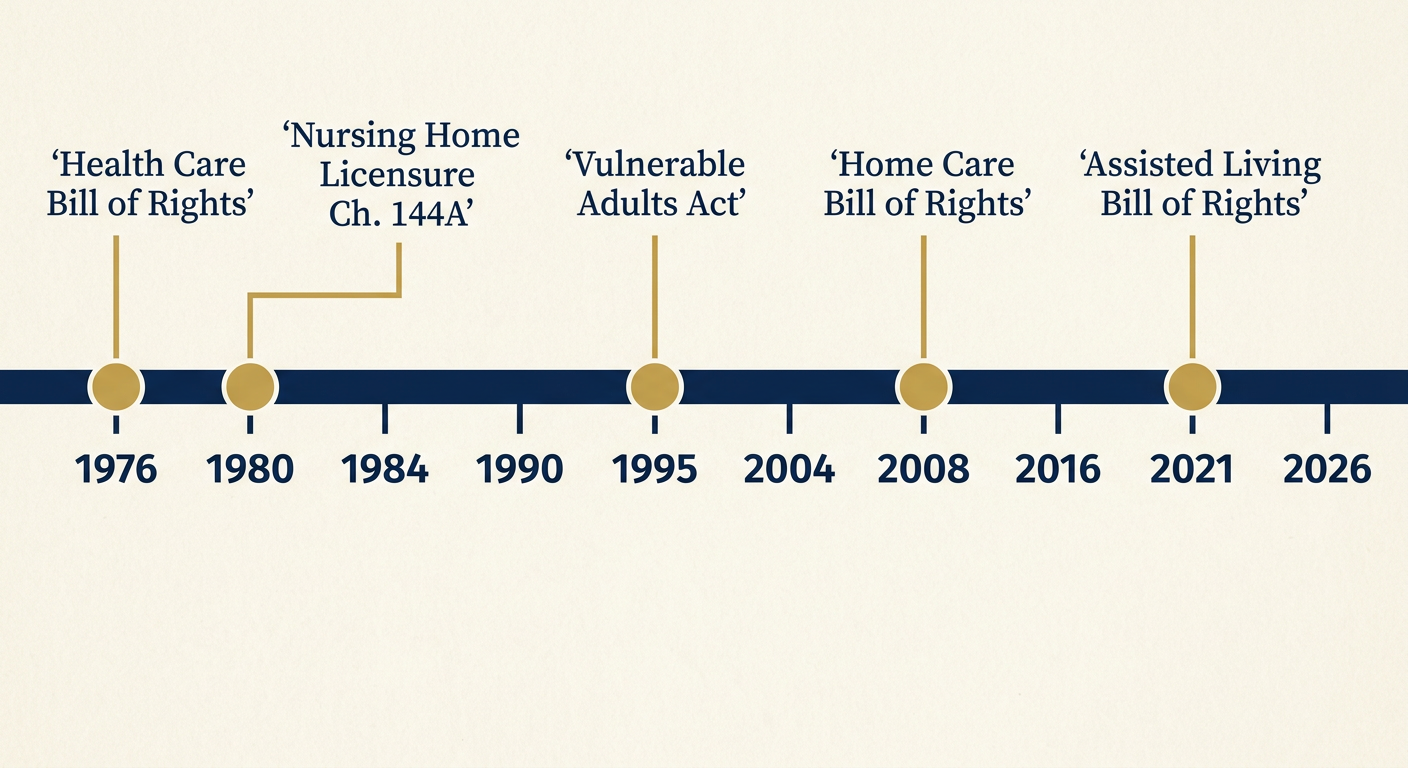
The legal framework behind the registry has been built in layers. Each statute below expanded either the list of protected residents or the reach of the investigative obligation. Knowing which framework applied on the date of harm is the first question in most cases.
| Year | Framework | What It Established |
|---|---|---|
| 1976 | Minnesota Health Care Bill of Rights | Minn. Stat. § 144.651: the baseline rights of any patient or resident receiving care in a Minnesota health facility, including dignity, informed consent, and freedom from unnecessary restraint. |
| 1980 | Minnesota Nursing Home Licensure | Minn. Stat. Ch. 144A: the licensing framework for nursing facilities, complaint procedures, and the surveyor authority that feeds the public violation record. |
| 1995 | Minnesota Vulnerable Adults Act | Minn. Stat. § 626.557: mandatory reporting of suspected maltreatment of vulnerable adults, including the investigative pathway that routes complaints through MDH and county adult protection. |
| 2008 | Home Care Bill of Rights | Minn. Stat. § 144A.44: the rights-of-care framework for home-care clients, including records access and service-plan-change notice. |
| 2021 | Assisted Living Bill of Rights | Minn. Stat. §§ 144G.90-.91 (effective August 1, 2021): the separate rights framework that applies to assisted-living facilities, long a gap in Minnesota oversight until the 2019-2021 reform package closed it. |
Outside the statutory framework, two other calendars matter. The default civil limitation under Minn. Stat. § 541.05 gives six years to file most residual claims. The comparative-fault rule under Minn. Stat. § 604.01 controls how fault is apportioned if the facility argues that family-provided care or third-party conduct contributed to the harm. Punitive damages require the separate pleading procedure under Minn. Stat. § 549.191.
Methodology
How This Registry Was Built
The registry is assembled from four source categories: Minnesota Department of Health Office of Health Facility Complaints investigative reports, CMS Care Compare federal survey data for Ramsey County facilities, Ramsey County adult protection public filings, and published state oversight reports and corrections-of-deficiency documentation. Every category in the table above is tied to a named public-record framework. Undocumented anecdotes and individual case narratives are excluded.
The companion methodology page explains the verification steps, the public-records request sequence through MDH and CMS, the records-access procedure under Minn. Stat. §§ 144.292-.293, and the subpoena mechanics under Minn. R. Civ. P. 45 for facility-held records that are not in the public file.
Transparency note: This registry is a living document. When MDH or CMS publishes new oversight data, or when a regulatory framework changes, the registry is updated and the change is noted in the freshness footer below. The registry does not republish specific facility findings; those are available directly at the MDH and CMS public portals.
Why This Registry Exists
Institutional Neglect Is a Clinical-Correlation Problem
Nursing home harm cases turn on the same engineering question that drives every serious injury matter we handle: can a subjective family concern be converted into an objective medical record that a reviewer cannot wave away? The answer depends on the clinical-correlation discipline. A family reporting that their mother seems confused and is losing weight is describing a concern. The same concern, run through the registry categories above, resolves into specific diagnostic work — a serum-albumin trend, a Braden Scale history, a urinalysis series, an imaging study that a defense-retained reviewer will have to explain.
That is why this registry sits inside the evidence-based methodology behind our personal injury practice as a Pillar II resource. The clinical-correlation pillar converts soft-tissue-style insurer defenses — "she was elderly, she was going to decline anyway" — into an argument that the decline has a named clinical pathway, a documented onset, and a preventable causation trail. The registry is the first step of that conversion: it tells a family which category their concern belongs to, which means it tells them which records to request.
The same discipline reaches adjacent evidence categories. Admission and discharge paperwork discipline is covered in the Regions Hospital trauma intake family checklist for families arriving at the emergency department after a facility incident. The emergency room bill upcoding and overcharge checklist sits on the billing side of the same record-request sequence. When the case involves causation and fault allocation, the Ramsey County liability decision tree for injury cases is the upstream logic companion. For the corridor-evidence analog outside the institutional-care setting, the Ayd Mill Road pothole and road decay timeline shows the same public-record-timeline discipline applied to road-surface evidence.
Where This Registry Applies
Related Services
Families using this registry are usually working toward one of two litigation lanes at our firm. When a resident has been harmed but is still living, the primary lane is nursing home abuse and elder neglect claims. When the harm has resulted in a resident’s death, the matter moves into wrongful death and fatal injury litigation, which carries its own statute-of-limitations and beneficiary-notice rules. Both lanes rely on the clinical-correlation work that this registry introduces.
Frequently Asked Questions
Common Questions About This Registry
Does this registry list specific facilities by name? +
No. The registry is a category-and-framework guide, not a facility-level ranking. Specific facility findings live on the Minnesota Department of Health portal and on the federal CMS Care Compare site — both of which are public and searchable. We publish the registry to help families understand what those portals are showing, not to duplicate them.
How do I request the medical record for my loved one? +
Under Minn. Stat. §§ 144.292-.293, a patient or their authorized representative can request the record directly from the provider, with defined response deadlines. The facility may charge a reasonable cost for copying. If the facility resists, the next step depends on the posture of the matter — for an active complaint, MDH investigators can compel review; for a litigated claim, a subpoena under Minn. R. Civ. P. 45 reaches records the facility will not produce voluntarily.
How long do I have to bring a claim for nursing home harm in Minnesota? +
The default limitation is six years under Minn. Stat. § 541.05 for most residual claims. Specific causes of action — medical negligence, wrongful death, statutory violations — have their own calendars that may be shorter. The sooner the record request and investigative sequence starts, the easier it is to preserve the clinical evidence before the facility overwrites or archives it.
What if the facility was assisted living, not a nursing home? +
Since August 1, 2021, assisted-living facilities in Minnesota have operated under a separate statutory framework: the Assisted Living Bill of Rights at Minn. Stat. §§ 144G.90-.91. The violation categories in the table above still apply conceptually, but the governing statute and the regulator are different. MDH licenses both, but the rules are not identical.